Genital Masculinizing
Welcome to Legacy Surgical Partners – we look forward to caring for you! Our priority is to make your surgery process and everything in between as pleasurable, empowering, and accessible as possible. Patients are expected to follow guidelines established by the WPATH Standards of care Version 8. We follow these standards—not as a gatekeeping hurdle—but as minimal guidelines that are useful guideposts that are protective. Though regret for gender affirming surgery is extremely rare, we are medical professionals who are here at your bequest. Surgery is irreversible, which puts the onus of responsibility on both patient and provider.
We're here to help you make essential decisions and know what to expect in surgery planning and recovery. Our team consists of:
- Surgeons
- A physician assistant
- Medical assistants
- Our surgery scheduler
- Office team
- And you
That’s right, you! We value your input, your perspective and all the work you are and will be doing to prepare for and recover from surgery. We look forward to getting to know you better and learning how we can help you.
We want to make your surgery and recovery as smooth as possible. We’ll answer questions you have and make sure you have the best possible outcome.
I. Metoidioplasty Overview
We know this surgery is extremely important. It takes incredible trust to allow a surgeon to perform this operation. We want you to know we are humbled by that trust and take it very seriously.
The first step in this complex process is understanding your options and creating a plan that meets your needs. We’ve created this overview to help you make important decisions and know what to expect.
What is metoidioplasty surgery?
Metoidioplasty (in Latin, “becoming male”) is a procedure in which we aim to both lengthen your penis and position it to be more forward-facing while maintaining full sensation. This procedure can be combined with urethral lengthening, scrotoplasty, hysterectomy and/or vaginectomy. Testicular implants and scrotoplasty, should these be desired, are accomplished in a second outpatient procedure. Goals:
- Give penis more length by releasing ligament attachment .
- Position penis to a more forward position.
- Remove, reposition, reshape local tissue to make penis more visible.
Each patient’s surgery and results are different.
II. Before Surgery
Before your first consultation, we encourage you to:
- Consider your goals and priorities for surgery.
- Write down your questions and bring them with you to your visit.
- Consider a support person to come with you. Ideally, this would be the same person who will care for you after surgery.
Your First Consultation
Your first consultation is an opportunity for us to learn about your hopes and goals. You may be given a questionnaire to help us meet your needs and measure the results. Your surgeon will review various surgical options and explain the process.
Once we understand your goals, we will:
- Evaluate your anatomy.
- Take pre-operative pictures.
- Assess your overall health to see which surgeries can meet your goals.
A fair amount of time is spent during the consultation with your surgeon, but you may also meet the other members of your care team.
Metoidioplasty Options
Simple Metoidioplasty
Scrotoplasty w/wo Implants
Urethral Lengthening
III. Preparing for Surgery
Metoidioplasty is a surgery that will limit physical activity for 2-6 weeks, depending on the type of procedure you have. A large part of its success depends on your preparedness. This means being in the best possible physical and mental health before the surgery.
Above all else, it is crucial to have reasonable expectations about what is possible for your body and what your surgeon can realistically accomplish. We recommend you:
- Speak with a mental health professional who has an understanding of gender care to help you navigate this process and exciting period of your life.
- Connect with peers who have been through this surgery for support. Please keep in mind that each person’s surgical plan, experience and result is unique. Information shared on some online forums may not be relevant to your surgery. Due to patient privacy laws, we never comment on another patient’s specific issues or experiences. We are happy to clarify anything related to your individual care.
This guide will help you meet the pre-surgery requirements, prepare for surgery and plan for your recovery. We are here to help ensure that your surgery is successful.
Maximizing Healing
You can expect that surgery will be stressful to your body and that this will require adequate time for healing. In the months and weeks leading up to surgery, maximizing your health—both mental and physical—will aid in achieving a swift recovery.
To optimize healing, we recommend:
- Getting roughly 0.5 gram of protein per weight in lbs a day to maximize healing (e.g. 150lb x 0.5=75g of protein per day).
- Reducing sugar and processed foods.
- Remaining active before having surgery. Keeping up with or adding a workout plan will benefit your overall health and support a speedy recovery. Examples can include adding daily walking, home yoga, or simple home workouts with body weight to your weekly routines.
IV. Planning for Recovery
We understand the importance and urgency of this surgery. We also know your success hinges on being well-prepared. Remember, this is a lifelong investment in your health. Optimal preparation can improve your chances of positive physical and mental health outcomes.
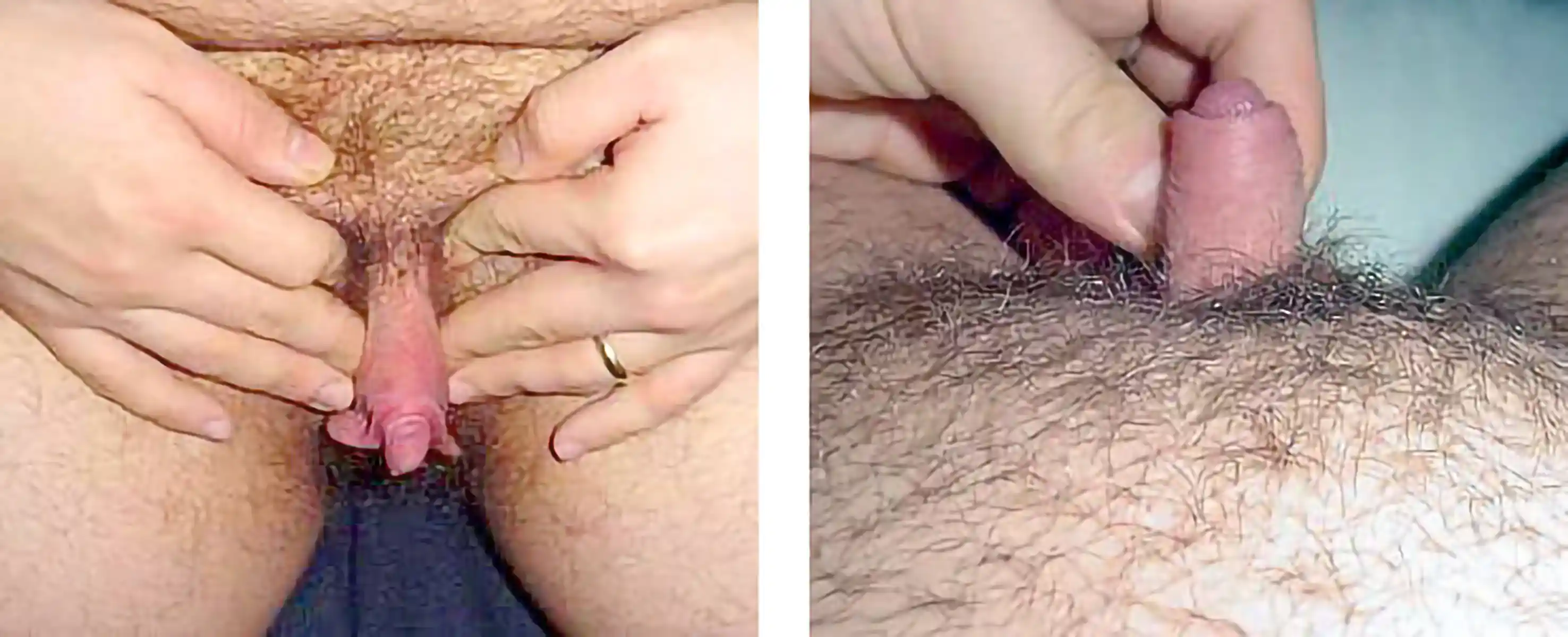
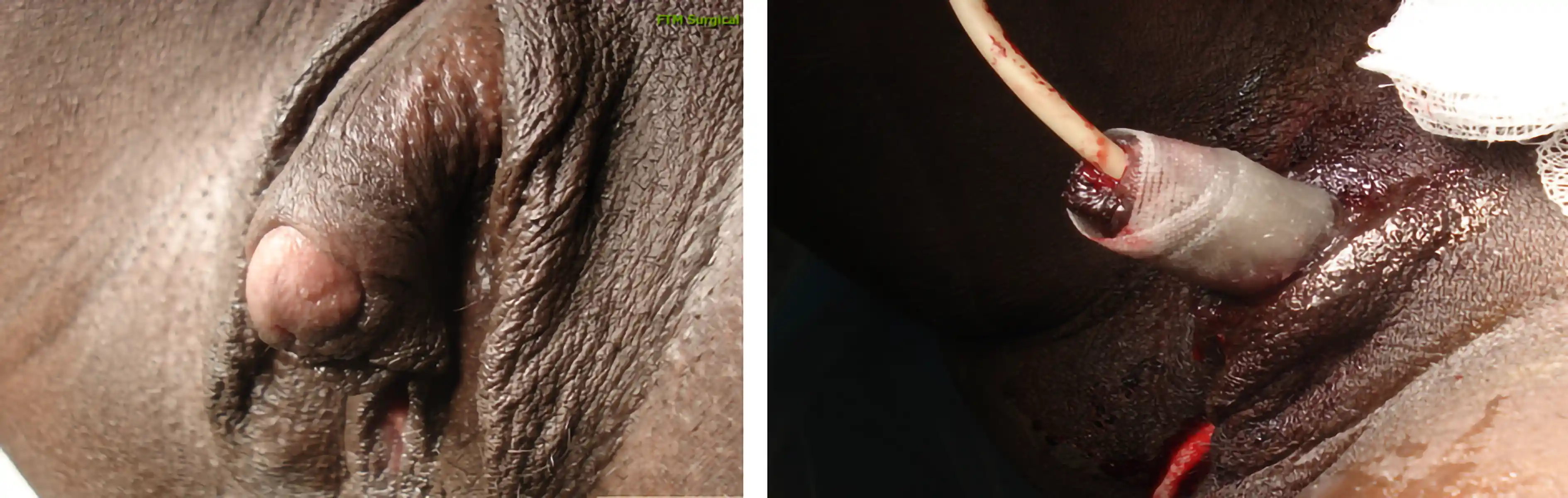
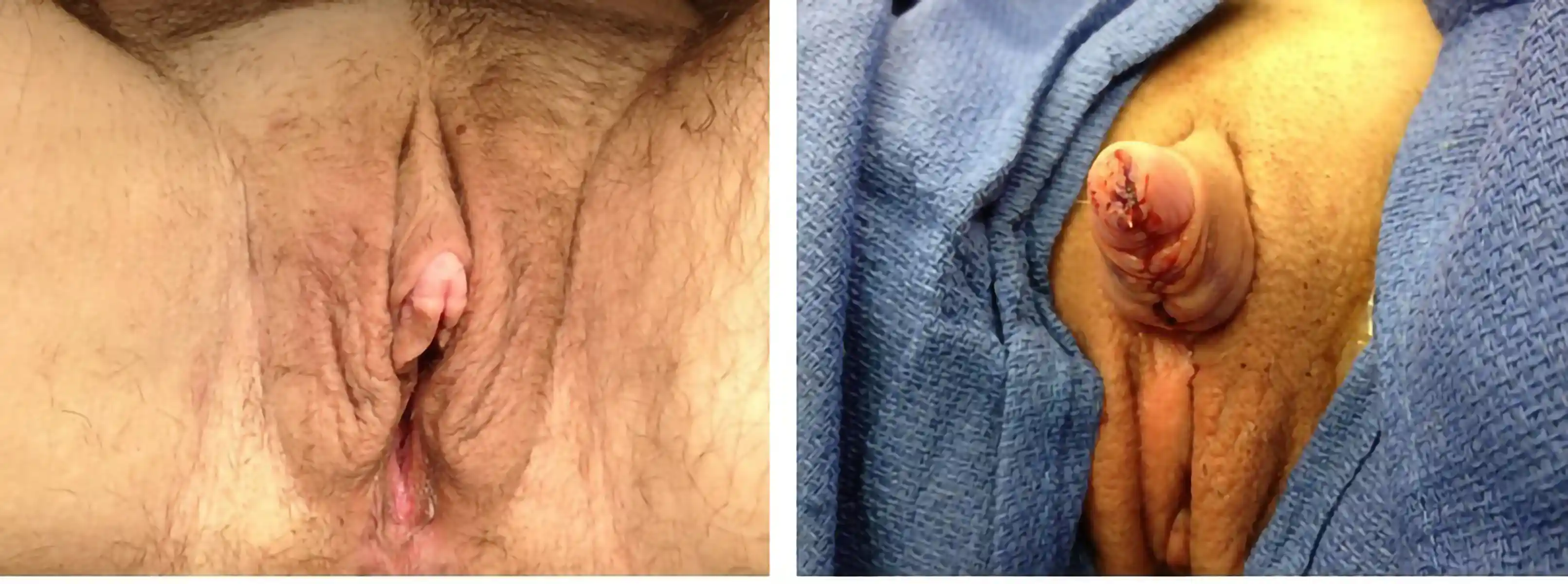
V. Surgical Results Gallery
Below are examples of genital masculinizing surgeries performed by our team. These images are shared with full patient consent and are intended to help you understand what to expect. They include pre-op and post-op views, which may contain nudity and surgical results.